
 |
| Joseph Goebbels |
The
“big lie” is a propaganda technique in which a falsehood is repeated so often and in
so many different ways that people come to believe that it is true. The term is generally credited to master Nazi
propagandist Joseph Goebbels. According
to Wikipedia, he wrote the following paragraph in an article dated 12 January
1941, 16 years after Hitler's first use of the phrase "big lie,"
titled "Aus Churchills Lügenfabrik" and translated "From
Churchill’s Lie Factory." It was published in Die Zeit ohne Beispiel.
The essential English
leadership secret does not depend on particular intelligence. Rather, it
depends on a remarkably stupid thick-headedness. The English follow the
principle that when one lies, one should lie big, and stick to it. They keep up
their lies, even at the risk of looking ridiculous.
The
technique has become commonplace in all sorts of marketing and is particularly
rampant in Pharmaceutical Company marketing.
It is part and parcel of the process of turning facts that have never
been established into established facts, as I wrote about in my post of January 31, 2012.
I of
course need to make the following disclaimer for any reader who is logic-challenged: Just because someone uses a propaganda technique
invented by the Nazis does not make them a Nazi. I am not calling anyone in
the pharmaceutical industry a Nazi, so don’t write me a letter.
I
have already done several posts on how drug companies have turned
irritability, temper tantrums, affective reactivity and other very normal
behaviors and emotions in children into symptoms of mania (or ADHD, or both).
In this post I will add one more, to show how often this nonsense is
repeated over and over again in poorly designed and misleading journal
articles, complete with plausible deniability, and then reported uncritically
in the medical press.
One way to propagate a lie about the effectiveness of pharmaceuticals is through the publication of studies in which subjects fill out self-report tests or are subjected to symptom rating scales based on their immediate presentation at the time they are seen. The results of symptom ratings scales are tabulated uncritically and produced in a journal article- as if the results of the tests prove something. I discussed some of the issues involved in symptom rating scales in my previous posts, Counting Symptoms That Don't Count, and A Stupid Study and an Even Stupider Headline.
A journal article called Age Group Differences in Bipolar Mania by Safer, Zito, and Safer was published online in the journal Comprehensive Psychiatry on June 12, 2012. As reflected in the title of the journal article, the psychiatric press dutifully but incorrectly wrote that the conclusion of the article was that symptoms of bipolar are different in children and adolescents with mania than they are in adults.
The study seemed to say that aggression, irritability and motor activity were more prominent symptoms in pre-teens than teens. Adolescents had more aggression and irritability than adults, while adults showed more grandiosity and hypersexuality. Proof positive that the symptoms said to be more common in teens and pre-teens were actually symptoms of bipolar disorder?
If you only read the news reports or superficially glossed over the abstract of the actual article, you might think so.
Notice how the authors cannot be accused of lying, since this is in fact what their study actually showed. The "take home message," however, is that this means that these symptoms are in fact valid symptoms of bipolar disorder in kids.
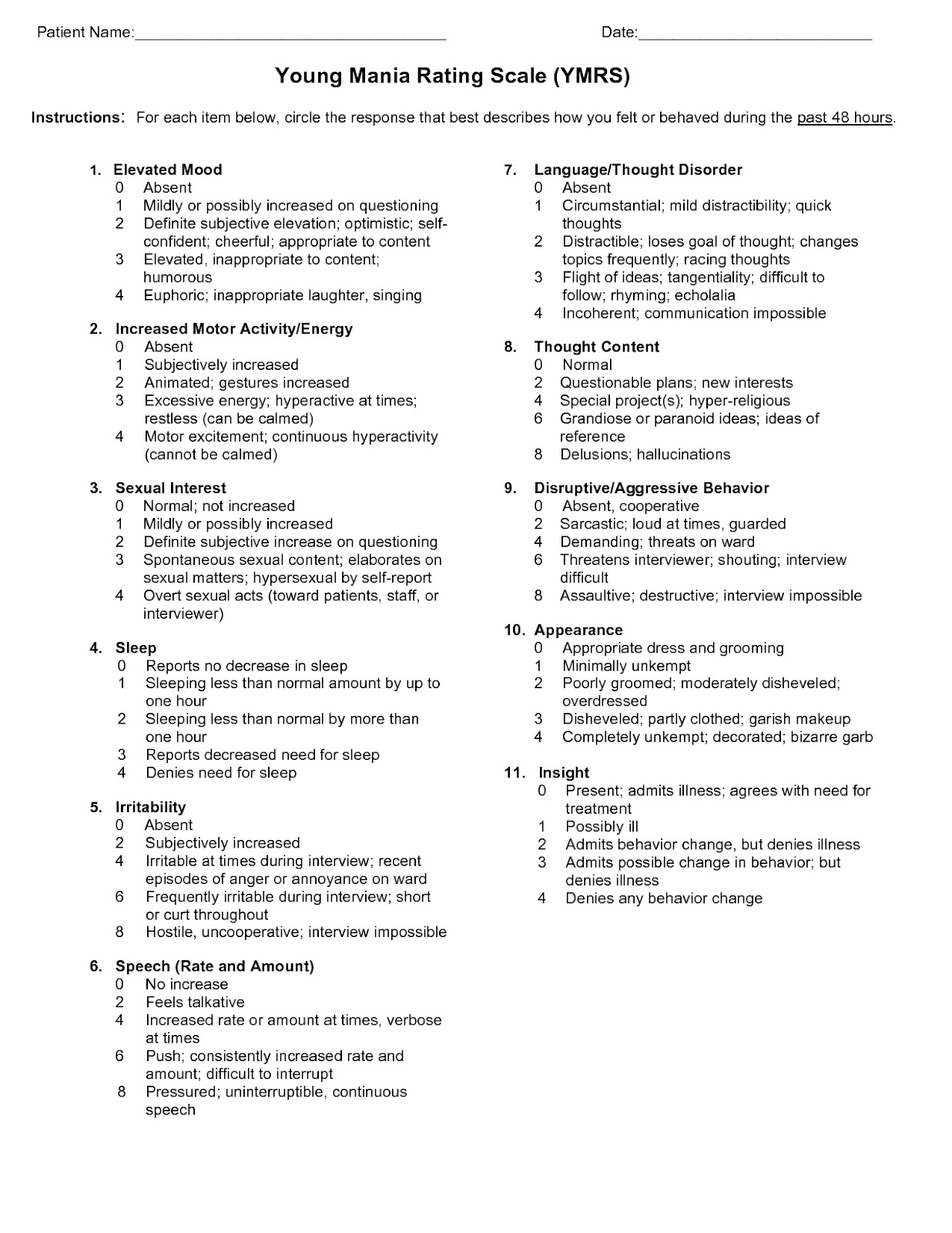
So let's take a closer look at the study and the YMRS. The study was based on a review of the literature describing several other studies, and the other studies that were chosen for review were "... studies reporting age group differences in total YMRS scores that included individual baseline item scores." So this study reviewed other studies that used what I will soon show is a highly suspect test.
1. To be screen out patients who for sure do NOT have the diagnosis and make sure that anyone who might have the diagnosis is included for evaluation. In other words, the tests are designed to have a lot of false positives, that is, people who score positively on the test but do not in fact, have the disorder.
The authors of this review clearly know that the YMRS is a screening instrument: "These outpatient studies required a minimum YMRS total baseline score of 20 for inclusion and achieved total baseline YMRS scores of 28 to 33 indicating at least moderate manic symptoms [20,22,23,25]. In these clinical trials sponsored by industry, trained raters did the YMRS item scoring at baseline. The subjects who met full research criteria for mania were subsequently randomized into placebo and medication treatment groups."
2. To measure changes in symptoms over time in patients who have already been diagnosed correctly by other means. The other means that are used usually consist of research diagnostic clinical interviews, but we have no way of knowing how well the clinical interviews were done - particularly whether the duration and pervasiveness criteria of the symptoms were applied correctly, since this is frequently not done by drug company shills.
But even using a symptom rating scale to measure changes in symptoms is frought with difficulty, particularly in the case of the YMRS, which completely ignores the issue of symptom pervasiveness and duration.
The problem with tests that ask patients to rate their own symptoms was described succinctly by one patient, who purportedly said about a psychiatrist who used a self report question as the entire basis for prescribing drugs, "The question is always the same. He asks me, ‘On a scale of 1 to 10, rate your mood.’ I answer, but you know, in 6 hours I might have a different answer.”
Many of these rating scales uses what is called a Likert Scale. Likert Scales generally ask a patient or a researcher to rate the severity of a given symptom on a 4 to 7 point scale. A big issue with Likert Scales in self-report instruments is that when they ask whether a symptom is mild or severe is that they do not indicate the answer to the question, compared to what? Compared to a patient with a clinical disorder, or compared to the symptoms as they have been experienced by the patients themselves? When someone is very sad but has never been clinically depressed, he might rate the sadness as severe. Having perhaps never seen another person with a severe clinical depression, he has no external reference point that would distinguish a normal mood from a highly abnormal mood.
Now for the YMRS. The YMRS asks a clinician to rate the patient's symptom based on what the patient looks like or says at the time of the interview. Let's look at item number 5 on the YMRS scale, irritibility. The interviewer is asked to rate it on a 5 point scale based on observations during administration of the test. 0 = absent, 1 = subjectively increased, 2 = irritable at times dring the interview, or recent episodes of anger or annoyance on the ward, 3 = frequently irritable during the interview: short, curt throughout, and 4 = hostile, uncooperative, interview impossible.
Notice that there is no requirement than an effort be made to find out why the patient presents with irritability during the interview. It just assumes that it is due to the underlying mania. But how long has it been going on? Just today? How do we know the patient is not acting irritable because he had been having a really bad day, or because the interviewer was perceived as condescending? We don't.
Or take item #6, rate and amount of speech. Manic patients have what we called pressured speech - they talk and talk and no one can get a word in edgewise. This is present regardless of external circumstances. If a patient exhibits very fast speech in the YMRS interview, on the other hand, the symptom could conceivably be present because the patient is in a big hurry to leave on that particular day, but characterologically likes to make sure the doctor gets a very precise answer with all its myriad details to any question.
Without this additional information, the answers to the questions are meaningless! In children, aggression and irritability have hundreds of potential causes besides their supposedly being symptoms of bipolar disorder.
But the mantra that they are indeed symptoms of bipolar disorder in children is once again subtly repeated. Over and over and over again: the big lie technique in operation.






The big lie effect might be related to the more general "Repetitio mater studiorum est" (Repetition is the mother of all learning). That older principle applies whether what we learn is true or false. Propaganda and good education often designate the same thing seen by differently minded observers.
ReplyDeleteYou convincingly pointed the flaws into that research article. But I am wondering if it was necessary to call it a "big lie" (i.e. fraud) rather than just bad/sloppy/flawed-research.
One reason I am dubious about the "lie" explanation is your counter-productive use of the Goebbles reference: Goebbles was abusively accusing the English of practicing the "big lie". So the propaganda tool demonstrated here is not so much repetition than vilifying the opponent (with accusations of being a repetitive liar). The logical conclusion is that we should avoid imitating Goebbles, and restrain ourselves from accusations of lying except in provable cases (other cases of false information might be explained by a combination of conflicts of interest, selection bias or sloppiness rather than plain dishonesty).
Mr. Holmes,
DeleteThanks for your comment, but I disagree. If the type of misleading "research" described here were a rare event, then I might consider calling it just a poor performance on the part of the journal article authors. But the bipolar disease mongering is rampant, with scores of these articles coming out all the time (In fact, there's a whole journal devoted to them, the Journal of Affective Disorders, whose editor is known pharma shill Hagop Akiskal).
These articles are often ghost written by the marketing departments of pharmaceutical companies. The medical profession has only recently started looking into this, and there is no doubt that this was a widespread practice.
The results of these studies are then cited over and over again in presentations to physicians by both pharma-linked academics and pharmaceutical reps, with a few phrases thrown in - that everyone ignores - to cover their asses. See my post - plausible deniability.
I can not give the folks propagating this bull the benefit of the doubt about their honesty. I've seen how they use old debate tricks to get out of answering honest questions about their work from their audience - I described a few examples in earlier posts.
Then there is the fact reported by The New York Times that Joseph Biederman, the worst of the bunch, promised the makers of rispirdal that his study would show it "effective" in "pediatric bipolar disorder" before he even did the study!
I appreciate your blogs, Dr. Allen. I first ran across you in searching out some answers as I was sytematically getting off more than 11 medications some four months ago. Only two of therect the time were actually prescribed for my "bipolar II." the others were to treat the side effects of meds like lithium which affected my thyroid and caused hand tremors.
DeleteI am not sure if I remember the exact event that was the catalyst for my withdraw from psych meds or maybe that it was a series of events. One thing I know for sure is in the six years after my "diagnoses" I was never stabilized. Ever.
The withdraw landed me in the hospital with some significant anxiety. I had finally run across a doc that enjoyed treating atypical depression. During that ay stay we determined that I was probably misdiagnosed since my moods didn't shift after dropping the last psych med.
Instead here is what has been determined. During the two years prior to my disgnosis (actually a few more years) I had been going through significant perimenopausal symptoms. My marriage was falling apart. My ex- husband and I lost jobs 8 months apart taking our income from $90k to under $20 k. We had to borrow money to pay bills, ran up credit cards, sold our house, moved, divorced, filed bankruptcy, lost a grandfather, a father-in-law, and my father. For the first time in my life I began to have unsafe sexual relationships. Many of them. I can remember sitting in the bathtub with water running over me almost catatonic.
When I finally ended up in the hospital I exhibited rapid speech and racing thoughts do bad I was sweating trying to talk as fast as mind was going. Diagnosis: bipolar II with borderline personality disorder.
The meds almost killed me. I attempted suicide for the first time I my life last summer (I am 53) after getting on Prozac for 3 weeks. I was not taken off any of the others except lithium.
To date, 4 months after starting my journey I have deleted 15 total medications. I am now on PremPro and an antiinflamitory med. no psych meds. No mood swings. Only a little anxiety left from the last med step off from 2 weeks ago which will go away as it has with the others.
Now I Begin the journey of rebuilding my life including health, finances while trying to get off disability, a lost career, broken family relationships (my mom has stopped contact for a year) and so on. I have thought of stating my own blog and public speaking but dont know where to start or what exactly my topic would be -- too many to choose.
So thanks for speaking out. Maybe it will help someone out there that might be headed down the road I have been take a detour.
Goebbels is known for this quotation but Hitler actually wrote it (or rather dictated it) in Mein Kampf almost twenty years earlier in describing the English media's writings during World War One and their effect (in Hitler's judgment) of turning world opinion against the Central Powers (mainly by reporting bogus stories of German atrocities, much like the the "Kuwaiti babies left to die in hospital" narrative which led in part to the first Gulf War).
ReplyDelete